When I received the ADA’s invitation to share my COVID experience, I was immediately reminded of the fall of 1964. It was the first day of the 8th grade, my last year in Junior High. This very memorable year began when the teacher invited - well insisted - that each one of us come to the front and share our summer vacation experiences with the class. I don’t remember a word I said, but I vividly remember being terrified.
A few weeks later, I fell from the roof of a garage and broke my right wrist. I was stuffing colored napkins into a chicken wire form on a sports queen homecoming parade float for my older brother’s girl-friend. I remember that the concrete driveway was very hard! It took a while to heal, but the cast was cool and besides being called stupid, I did get some sympathy. However, what would make it a most memorable year was graduating in June of 1965, because my next step was High School and that was a big step. But that is not what made it really memorable, either. After the graduation ceremony, my brother, parents, and grandparents walked out of the school gate and what happened next was burned into my memory. My grandfather dropped to the sidewalk and died from a heart attack.
So why is this ancient history relevant to this monograph article? Well, let me explain:
I didn’t sleep well the night before I drove to a conference. When I got up that morning, my neck and my left arm were a little achy. It was February 28, 2020, the first day of a Dentsply Sirona SureSmile conference in San Diego. I was looking forward to learning how to make in-office aligners with my new Sprint Ray Pro 95 3D printer. I didn’t know it then, but that day would prove to be another memorable day in my life.
While attending, I was experiencing my own heart attack. Like a typical guy, I maintained my denial - I didn’t sleep well the night before, I was cramped in the lectures, my neck was sore from doing dentistry and that is why my arm hurt, etc.
I drove home and stopped at my office to pick up a case for a consultation the next morning at the conference, took a few hits of some O2 and drove home. An hour later, I felt like a screwdriver was going into my chest, through my heart and coming out my back. I told my wife that I was going to the hospital and she could call our daughter to give her a ride. I wasn’t waiting, I was going. Now!
The next day, I had a stent placed, got some lectures on my lousy diet and was instructed to take a week off before returning to work. March 9th was my first day back, and all was good. I dodged a bullet. After that first week, I decided that I didn’t want to work so hard anymore. My three day, Monday through Wednesday schedule was hectic, so I made the decision to lighten the load, reluctantly letting my second assistant go. Three days later, on March 16th, the COVID lockdown hit and like everyone else, we closed the office indefinitely. I was filled with mixed emotions.
Recovery
The first week off was a little stressful from the uncertainty but strangely relaxing at the same time. I could see that I was going to have some unanticipated recovery time. Then I thought I was going to get some much needed freedom to finish writing my third book, which was about 2/3 completed.
As it turned out, that wasn’t going to happen. The reality of the financial stress facing my business sank in. What would happen to my business and my livelihood? I wasn’t ready to hang it up and retire just yet.
Along with my staff, I searched online for any information and guidance I could find. I watched and listened to many hours of CE courses, many from ACT Dental. We were all full of questions and concerns. I took the step of temporarily laying off my remaining staff so they could draw unemployment. However, I kept my office manager, Debbie, on the payroll so she could answer the phones and repeatedly rescheduled patient appointments. She also began to assemble all of the guidance we could find and laid out the protocols for reopening. From home, my assistant, Danielle, kept trying to order the elusive PPE and supplies we needed to prepare for safe reopening, whenever that would be.
Innovation Begins
With much time to search e-mails and spend time online, I looked for solutions to mitigate the potential spread of airborne pathogens. It appeared to me that COVID originated in China and all the solutions I found online also seemed to be from China. It seemed very suspicious to me. However, I did find some solutions which intrigued me. I thought, “These are great ideas, but I can do better.”
With that thought in mind, I embarked on what would become a 6 month project to “reinvent the wheel.” I became focused – my wife would say obsessed - with the project. The only interruptions would be gathering information to repeatedly applying for SBA and PPP loans and grants and the seemingly endless waits while being placed on hold. One call was kind enough to inform me that there were 864 calls ahead of me. Amazingly, it was only a 2.5 hour wait! But, let’s get back to the project.
Figure 1: Dentistry By Design Training Facility
When I first built my office from 1998-2001, one of my main objectives was to create my Dentistry by Design training facility in which I could teach doctors the best usage and procedures for creating esthetic CEREC restorations (Figs 1 & 2). In 2004, I published a book on the subject, Highly Esthetic CEREC Solutions.
Figure 2: Doctors Learning CEREC Procedures
The office design included two central vacuum systems, one for traditional floor vacuuming. The second system was for dust collection generated from work on typodonts, CEREC powdering and porcelain grinding in the training facility. These systems kept our environment as free of airborne debris as possible.
The concept of my “reinvention” project was to meld my central vacuum systems with a patient aerosol collection system. I saw several systems online which offered the collection of aerosols, but they reintroduced the filtered air back into the room. Although they claimed a 99% kill rate, I didn’t want any of the air recirculated into the room. I also didn’t want to give up floor space for another piece of equipment. I determined to have a solution that removed the potentially infectious materials from the office environment, but I also wanted a fixed installation in each of my five treatment rooms.
I began by sourcing the required components. The first step was to find a collection device. I researched a number of hoses and tubing options, discovering a perfect solution at a woodworking site. A company offered a 2” sectional pipe which could be assembled in any length and maintain its position without drifting. To increase the area of collection, a 6” diameter funnel could be fitted to the pipe (Fig 3). Later, I was able to source a replaceable filter material which could cover the opening, collect moisture, and prevent things like articulating paper from entering the pipe. I was also able to locate barrier material that could be changed between patients to cover the portion of the collection pipe within the splash zone.
Figure 3: The EVADE™Collection Tube and Nozzle
Even though I was going send the air outside, I wanted to filter it to the best of my ability. I didn’t want the vacuum and collection piping to become a breeding ground for disease. Since my collected air would be ejected from the office, I reasoned that UVC light and Ozone would be a perfect pairing. They would keep the inside of my device and the vacuum pipe clear of potentially infectious material.
Ozone is excellent for killing pathogens, but not appropriate for injection into the occupied environment of the treatment room. For external venting, Ozone would be perfect. I researched UVC germicidal sterilization bulbs which also generated Ozone and found a socket and ballast to power the bulb. To complete this portion, I sourced filters to trap any particulates and debris that might escape treatment from the UVC/Ozone chamber and found a compact, replaceable HEPA filter which would do the job.
I had to consider the use of the device within multiple treatment rooms at the same time. If I provided a continuous connection to the vacuum for each of the devices, the vacuum flow of air would be greatly compromised. A valve would be necessary. A 2 ½” dust collection “blast gate” met that requirement.
The entire device required remote control so the operator could operate the unit easily. This was accomplished by modifying an off the shelf, plug-in remote lamp module and incorporating the transmitter fob into an old intra-oral camera foot pedal. I placed a manual on/off button near the assistant side as well for convenience.
3D Printing the Protoype
I chose ABS plastic to create my prototype “black box” because it was inexpensive, strong and easy to handle. Once the components were in place, the container and mounting/holding components had to be designed.
My 30 years of using the CEREC system made me very comfortable working in 3D. I found Rhinoceros, a 3D software design program, to create the components. With it I was able to design a frame for holding the HEPA filters, a mechanism for controlling the blast gate and activating the vacuum system and connecting the vacuum pipes.
Just a few months earlier, I received delivery of my new 3D SprintRay Pro 95 printer, and got training 2 weeks before my heart attack. I did not have an opportunity to use the printer before the lockdown hit, so I brought the printer home to try and print some of the components I needed for the project. Through trial and error, I got quite an education and a lot of practice doing 3D design and printing.
Over the next three months, I spent 8-10 hours a day sourcing, designing, assembling and testing every aspect of the project while viewing and listening to CE courses. My COVID “vacation” was very busy!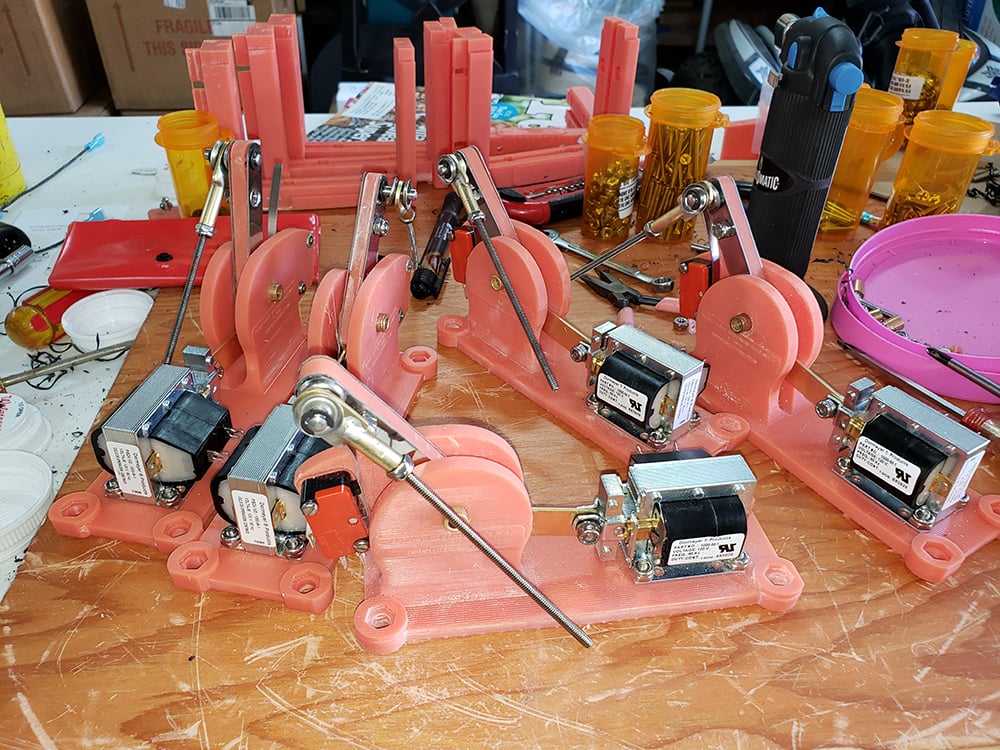
Figure 4: 3D Printed Actuator Prototypes
An actuator device was needed to open and close the blast gate which would in turn activate the vacuum system as needed (Fig 4). Figures 5 & 6 show the HEPA filter frames and other parts which were 3D printed.
Figure 5: Filter Frame and Other Orange 3D Printed Parts
Figure 6: Assembled Countertop Prototype
The next step was for me to install a dedicated 280 CFM, dual motor central vacuum system (Fig 7), placing over 100 feet of vacuum pipe and wiring in the ceilings and walls. Finally, I mounted a black box prototype on the 12 o’clock cabinet in each of my five treatment rooms.
Figure 7: 280 CFM Central Vac Unit
On June 1, 2020 we reopened our office for patient care and put the EVADE™ (Externally Vented Aerosol and Droplet Evacuation) system to work.
I used my 3D program to design custom ¼” sneeze guards across my front desk to protect staff and patients alike (Fig. 8). I sent the designs to a local plastics fabricator who used their CNC machine to cut the panels and supports. I was able to install them with no drilling or hardware because it is a self-supporting pressure fit (Fig. 9).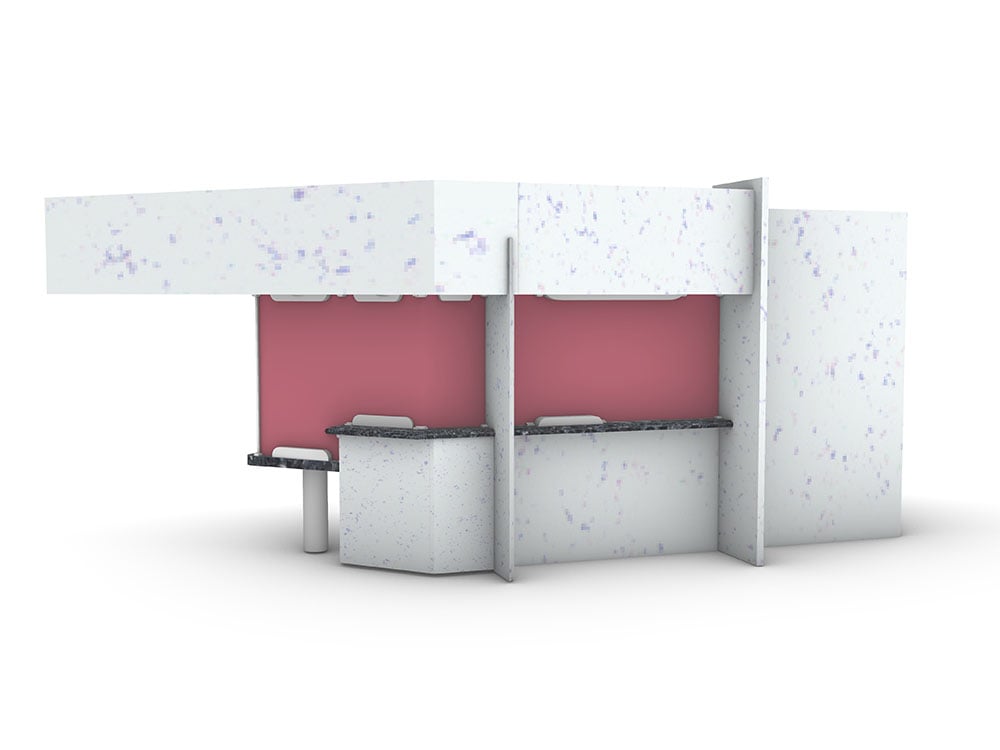
Figure 8: Front Desk Barrier Design
Figure 9: Front Desk Barrier Installation
After a few weeks of use, I was able to identify areas for improvement to the EVADE™ prototypes. I set out to create final versions mounted to my dental unit and controlled by a remote foot pedal or a physical on/off switch. ABS plastic degrades under UV light so I chose an opaque white UV resistant Plexiglas for the final housing.
3D printing allowed me to manufacture bulkhead connectors for each end of the collection pipe (Fig 10), and a camshaft for a linear actuator which operates the blast gate. This allowed for sequential activation of two micro switches, one of which controls the vacuum system. The other switch controls the UVC/Ozone bulb causing it to remain lit for several seconds after the vacuum flow has stopped (Fig 11). In this way, the surface of the HEPA filters are irradiated, killing any pathogens lingering in the light chamber.

Figure 10: EVADE™ - Dental Chair Post Mounting Apparatus
Figure 11: EVADE™ - Pole Mounted
Figure 12: EVADE™ - Service Access
The installed EVADE™ system does not occupy any floor space (Fig 12). It looks like it has always been a part of the dental chair assembly, but still opens up the opportunity to market our efforts to our grateful patients (Fig 13).
Figure 13: The EVADE™ System Ready For Patient Use
I wanted to pursue the process for patenting the device and did some online research. I explored a provisional patent on Legal Zoom and found it to be fairly easy, but I wanted a full patent. A friend referred me to a patent attorney who told me that his retainer fee would start at $10,000 plus patent fees, corrections, drawings, etc. That was a shock, so I went to the USPTO website and became even more confused. However, I did register as an agent, so I could eventually file myself. After reviewing the process, I put it on hold and turned my attention back to my office.
Positive Pressure A/C
As an additional level of prevention, I had my HVAC contractor install a positive pressure air system to bring outside air into my hallways with externally vented fans in my treatment rooms. This system creates 8.5 air volume changes per hour in a direction away from the patient. All of my patients are very pleased with the extra level of care and precaution that we provide for their dental care experience.
Collection and external venting of aerosols and a positive pressure air circulation system provides protections for the health of patients and staff alike. They should both be standard in every dental office. External venting of collected aerosols with the EVADE™ system is the best possible solution and is applicable to any industry which deals with patient generated aerosols. The COVID crisis has prompted the creation of this solution which should become a standard of care even after COVID.
The Patent
Now that everything at the office was stabilizing and our protocols were starting to become routine, I began to think of ways to let our patients know about what we had put in place for their benefit. However, I knew that as soon as I made the EVADE™ system public, I would lose my opportunity to secure a patent, so I got serious about it.
It took nearly two months to figure out what I needed to do, understand the documentation requirements and put it all together. Finally, I was able to navigate the onerous patent process without an attorney and apply for a non-provisional utility patent for the EVADE™ System. To my amazement, just 3 months later, my application was accepted and EVADE™ was granted a patent that was issued on 3/23/2021.
I then turned my attention to ways in which I could best communicate the benefits of EVADE™ to my patients and potential new patients. I had already completed the 3D models of the device, so I applied my new found skills to creating a 3D office environment and treatment room. Not satisfied with static images, the next step was to explore animation of my 3D models to demonstrate EVADE™ in action. It took nearly 300 hours of design, experimentation, conversations with tech support and rendering to arrive at a “realistic” animation. I imported the animation into my video editing program, added some graphics, a narration and a sound track to complete the project which I posted to my website at https://EVADEsystems.com.
Our office protocols have forced a reduction in the number of patients in the office at a time, but our protocols have also given us the opportunity to bring a much higher level of personalized care to our patients. The front desk enclosure, the positive pressure air flow system and the EVADE™ system all spark a great deal of conversation with our patients and clearly demonstrate to them just how much we care for their health and well-being. Case acceptance and demand for treatment has risen as a result. Our productivity has surpassed our pre-COVID levels while providing more attention to our awesome patients.
The pressure that COVID created has been a game changer throughout the world. All of us have been impacted by this new world order and it seems that nothing will ever be the same. However, through innovation and determination, we will overcome the obstacles, just like my doctors and the amazing stent they placed to allow me to continue on.
__________
Dr. Rich Masek
Dr. Rich Masek is an AGD Fellow and Accredited with the American Academy of Cosmetic Dentistry. He maintains a private practice in San Diego, CA.
