Improved understanding of the dental caries process and how to manage risk have led to the development of practical “4D” tools to help prevent and control caries. (The articles in this series were presented at a symposium and did not undergo peer review.)
ABSTRACT
Background: This report provides an overview of dental caries in 2021, with an emphasis on how current research on epidemiology, etiology, and early detection fits with evidence-into-action initiatives across multiple stakeholder domains.
Methods: This overview, based on recent reviews and reports from the international literature, highlights key shifts in thinking about caries and explores related implementation and policy activities pertaining to caries classification and management.
Results: It is important to understand the scale of untreated caries as a continuing global problem for adults and children, as recognized in the 2021 World Health Organization resolution on oral health. Changes in our understanding of the caries process and its interaction with the oral microbiome have led to an appreciation of caries as a noncommunicable disease and enable caries control by maintaining the ecological balance between health and disease. Early detection of caries is now seen as a vital component of caries assessments in both public health and clinical practice. The evolution of integrated caries classification and management systems has led to a focus on a holistic, patient-centered, long-term view of caries management, monitoring, and outcomes. These findings have informed a range of evidence-into-action activities that have the potential to improve health and treatment in a post–COVID-19 world, as we move toward making cavities history.
Conclusions: Integration of new and existing concepts of caries offers novel ways in which prevention can be achieved and care provided for populations and individuals to maximize health outcomes while minimizing surgical intervention and aerosol generation.
Practical Implications: Improved understanding of the dynamics of the dental caries process, together with enhanced understanding of how to manage risk and create a balance between health and disease have led to the development of practical “4D” tools to help prevent and control caries in clinical practice with a minimally interventive approach associated with less aerosol generation.
BACKGROUND AND METHODS
As a prelude to a series of more focused articles, this report provides an overview of dental caries in 2021, with particular emphasis on how current research evidence on epidemiology, etiology, and early detection fits with recent international evidence-into-action initiatives taking place across multiple stakeholder domains.
This overview, based on peer-reviewed articles and reviews drawn from the international literature, highlights key shifts in thinking about caries, ranging from terminology to disease concepts, care planning, and public health implications. It also explores recent implementation and policy activities pertaining to caries classification and management and highlights how the COVID-19 pandemic is now driving the adoption of minimally interventive caries management and prevention linked to the first World Health Organization (WHO) oral health resolution in 14 years.
Evolution of terminology and concepts
Repeated discussions among researchers, clinicians, public health professionals, and policy makers regarding the most appropriate terms to use to describe conditions and characteristics of dental caries and related matters prompted the European Organisation for Caries Research (ORCA) and the International Association for Dental Research (IADR) Cariology Research Group to hold a joint workshop in 2019 in Frankfurt, Germany.1 Workshop participants selected commonly used terms and reviewed their definitions, based on current concepts and science, and then agreed by consensus (through blind voting) on the most appropriate terms and definitions. The definition of “dental caries as a disease” (with 100% agreement) was the following1:
Dental caries is a biofilm-mediated, diet modulated, multifactorial, non-communicable, dynamic disease resulting in net mineral loss of dental hard tissues . . . It is determined by biological, behavioral, psychosocial, and environmental factors. As a consequence of this process, a caries lesion develops.
The definition of “caries care/management/control” (again with 100% agreement) was this1:
Caries care/management/control are actions taken to interfere with mineral loss at all stages of the caries disease . . ., including non-operative and operative interventions/treatments. Because of the continuous de/remineralization processes, caries control needs to be continued throughout the life course. The terms caries care/management/control may be more appropriate than the term caries prevention.
The definition of “caries prevention” (with 88% agreement) was as follows1:
Caries prevention traditionally meant inhibition of caries initiation, otherwise called primary prevention. Primary, together with secondary and tertiary prevention, comprising non-operative and operative treatments, are now summarized under Caries care/management/control.
These definitions are based on both current concepts in the scientific literature and on experts’ opinions. The IADR and ORCA groups stated that the “suggested terminology is recommended for the use in research, in the public health field, as well as in clinical practice.”1 Such terminology and the concepts behind the definitions are markedly different from those taught to researchers, clinicians, and dental public health staff in earlier decades and represent a challenge to many stakeholder groups.
RESULTS
Epidemiology
The evidence base on caries detection and assessment has developed over many decades and the current concept of including clinical visual information on both enamel and dentin caries detection is not new.2-4 Key findings were published in the 1950s, 1960s, and 1970s, but there has been, in many countries, a failure to understand or implement these research findings. The newer guidance regarding epidemiology and clinical practice is, in fact, based on many decades of research.
Unfortunately, there are serious challenges associated with maintaining robust and reliable estimates of caries prevalence internationally, as well as understanding estimates of preventive and restorative care needs. These challenges stem from a limited understanding of the impact of caries detection thresholds in dental caries epidemiology. Figure 1 shows the proportion of 15-year-old adolescents from a 2013 survey of child dental health with dental caries at a range of detection cutoffs.5,6 These thresholds are based on the International Caries Detection and Assessment System (ICDAS) criteria,7-9 which range from codes 1 and 2 (initial-stage caries) to codes 3 and 4 (moderate caries) and codes 5 and 6 (extensive caries). These are the same thresholds used in the American Dental Association Caries Classification System.10 Figure 1 shows that if only traditional estimates of dental caries are used (ie, only open cavitated dentin caries [ICDAS 5 and 6]), 11% of the adolescents are considered to have had caries. However, if dentin lesions with shadows under the enamel (ICDAS 4) and cavitated enamel lesions (ICDAS 3) are included, 21% to 25% of the population is considered to have had caries. If the clinically relevant and potentially reversible initial stage lesions are included (including the noncavitated enamel lesions [ICDAS 1 and 2] found on examination in the field), then the percentage of adolescents with caries dramatically increases to 52%.5,6 Collection of caries data using this ICDAS-based system allows greater insights for both epidemiology and clinical practice11; it also enables the identification of clustering to inform population caries prevention strategies.12
Figure 1
Dental Caries Epidemiology: Impact of detection thresholds, 15 yr olds
The prevalence of initial stage-caries across populations is high and often not quantified
(Data on 15 year old children from 2013 National Child Dental Health Survey (CDHS) of England, Wales & NI)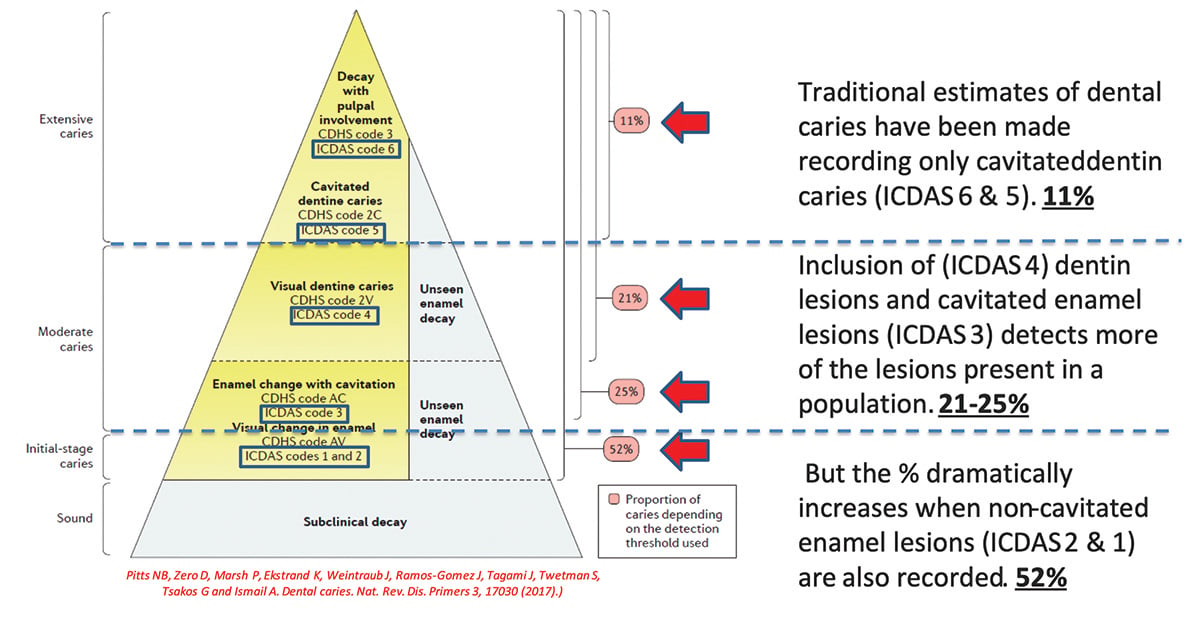
Pitts NB, Zero D, Marsh P, Ekstrand K, Weintraub J, Ramos-Gomez J, Tagami J, Twetman S, Tsakos G and Ismail A. Dental caries. Nat. Rev. Dis. Primers 3, 17030 (2017).
The significant variations associated with different surveys in different countries using different caries detection thresholds (let alone variations in sampling methods and training and calibration of examiners) compromises our ability to make international or regional comparisons. This has been demonstrated in many parts of the world, including Europe13 and Latin America.
Figure 2 provides an overview of caries epidemiology on a global level. The classical WHO criteria, which is compatible with the National Institute of Dental and Craniofacial Research criteria, only includes caries at the dentin cavitation level; data using these criteria are now more rarely collected or updated in valid national samples. Therefore, it is more difficult to assess genuine geographic variations in caries levels. In any case, these types of surveys systematically underestimate the true disease prevalence when initial (noncavitated) lesions (ICDAS 1 and 2 stages) are included (Figure 1). To try and address these issues, 3 organizations in Europe agreed to support a “Brussels Statement” on caries epidemiology,14 which sets out needs for modern criteria, together with the ability to compute backwards compatible data estimating what the prevalence of caries would have been if traditional criteria had been used. The statement advocates the inclusion of initial lesions scored by trained and calibrated examiners.14
Figure 2
Overview of Caries: what we know and what we don’t know
- Classical “WHO” (and NIDCR) “cavitation” data now more rarely collected/updated on valid National samples. These in any case systematically underestimate disease prevalence compared to when initial (non-cavitated) lesions at ICDAS 1 & 2 stages are also included (National Survey example from the “UK”)
- “Brussels Statement” sets out needs for modern/backwards compatible Epidemiology, advocates inclusion of initial lesions
- Global Burden of Disease Data increasingly important and used, measures caries by its impact on individuals
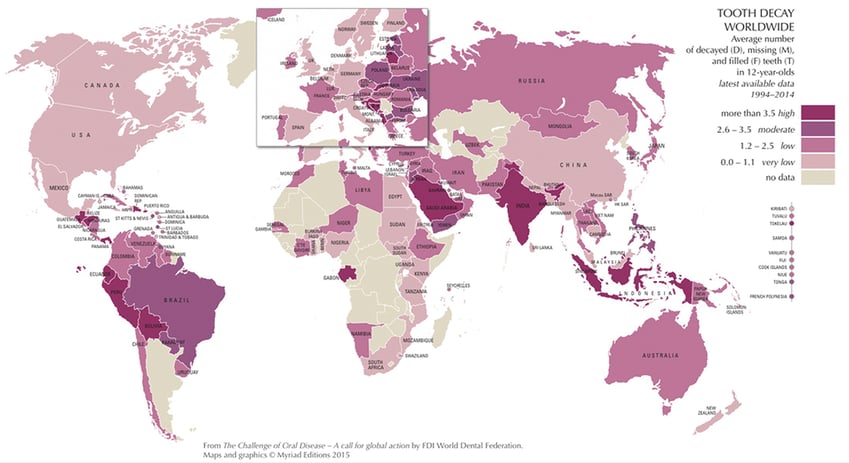
Selwitz R H, Ismail A I, Pitts N B. Dental caries. Lancet 2007; 369: 51-59. Pitts NB, Zero D, Marsh P, Ekstrand K, Weintraub J, Ramos-Gomez J, Tagami J, Twetman S, Tsakos G and Ismail A. Dental caries. Nat. Rev. Dis. Primers 3, 17030 (2017). Pitts NB, Eaton KA and Tsakos G. Brussels Statement on the Future Needs for Caries Epidemiology and Surveillance in Europe. Community Dental Health. June 2018 Volume 35 (2): 66. doi: 10.1922/CDH_PittsBrussels01
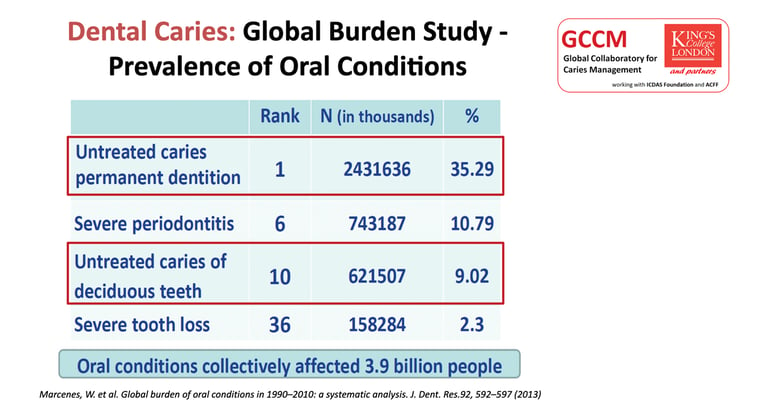
Over the past decade, inclusion of oral health data in the wider global burden of disease studies has provided a method of looking at caries prevalence based on the burden of caries as assessed by disability-adjusted life-years.15 These data are increasingly important and used in policy and planning as measures of the disease according to its impact on individuals. Clearly, caries is a chronic disease that extends into adulthood16; untreated caries in the permanent dentition ranked No. 1 across all oral conditions, affecting 35.29% of individuals, and untreated caries in primary teeth ranked No. 10 across all oral conditions, affecting 9.02% of individuals. Therefore, it is important to understand the scale of untreated caries as a continuing global problem, with health, economic,17 and social burdens for both adults and children. These issues have been explored in more depth through the Alliance for a Cavity-Free Future (ACFF) and its global consensus on policies to make cavities history.18,19
Etiology
The etiology of dental caries is complex, the understanding of which has evolved over the past 15 years.1,2,4 A recent review of dental caries aimed at researchers across a range of scientific disciplines4 generated a useful infographic, part of which is shown in Figure 3. This infographic demonstrates the interaction over time between the ecological community of bacteria at specific sites within the oral biofilm, producing organic acids by metabolizing dietary carbohydrates, and the tooth surface and subsurface on which results episodic demineralization and remineralization of the tooth, saliva, and any available fluoride. Our understanding of the caries process and its interaction with the oral biofilm/microbiome has changed over time. Rather than implicate specific organisms as the only way in which caries can be initiated or can progress, there is now an appreciation of the importance of maintaining a healthy environment at the tooth surface. Increased sugar intake, more frequent acid production, and changes in the pH at the tooth surface drive an ecological shift to a more pathogenic biofilm.4 Knowing that the environment can drive the caries process offers new opportunities to intervene to maintain health. Moreover, dental caries is now considered to be a noncommunicable disease,20 which has important policy implications.18,19
Figure 3
Summary Overview of Aetiology of Dental Caries
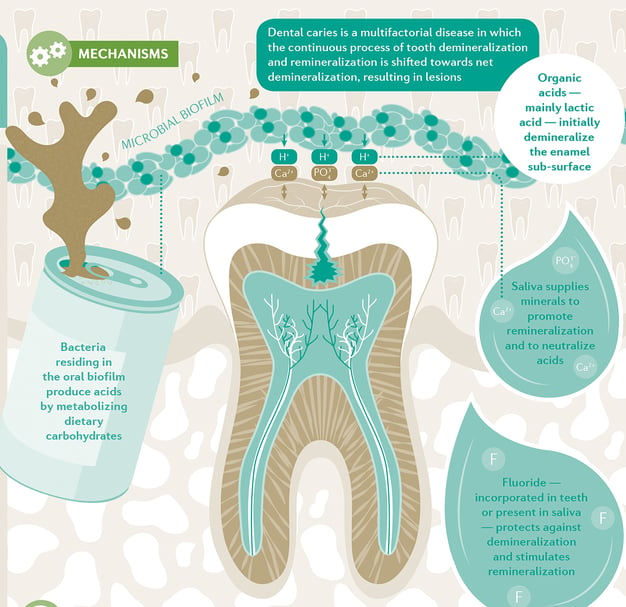
Pitts NB, Zero D, Marsh P, Ekstrand K, Weintraub J, Ramos-Gomez J, Tagami J, Twetman S, Tsakos G and Ismail A. Dental caries. Nat. Rev. Dis. Primers 3, 17030 (2017).
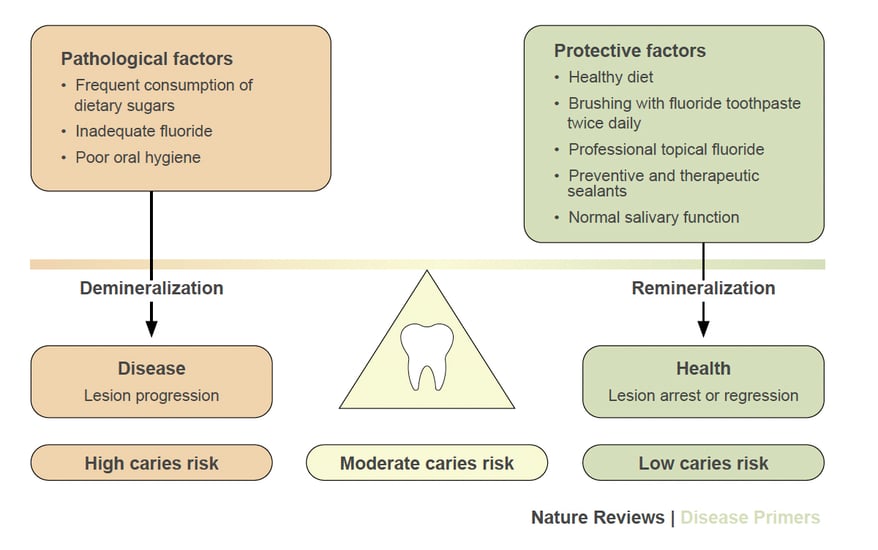
Consequently, in understanding and controlling dental caries, an increasing emphasis is being placed on balancing pathologic and protective factors. Figure 4 presents the pathologic factors that lead to demineralization and the balancing protective factors that lead to remineralization and lesion arrest or regression. This biological balance of factors has led to an enhanced appreciation of achieving caries control by maintaining the ecological balance between health and disease.
Figure 4
Balancing pathological and protective factors in dental caries
 Pitts, N.B. et al. (2017) Dental caries. Nat. Rev. Dis. Primers doi: 10.1038/nrdp.2017.30
Pitts, N.B. et al. (2017) Dental caries. Nat. Rev. Dis. Primers doi: 10.1038/nrdp.2017.30
Detection, measurement, and monitoring of lesions
A complete description of the evolution of caries classification systems is beyond the scope of this report, but it has been documented elsewhere.2-4,7-9,21,22 In summary, the ICDAS system was developed in 2002 “to produce a harmonised, evidence-based, international, system to lead to better quality information to inform decisions about appropriate diagnosis, prognosis and clinical management at both the individual and public health levels.”7 The system was developed in response to the widespread inability to compare results from different studies that used incompatible diagnostic criteria. From the start, ICDAS was designed to be applicable to epidemiology, clinical practice, research, and education. The system enables clinicians to detect lesions at various histologically and clinically meaningful stages, assess the activity of each lesion at a specific point in time, and then facilitate monitoring of lesions over time.23
To advance work in this field internationally, in 2013 the Global Collaboratory for Caries Management was formed as an umbrella group to facilitate delivery of preventive dental medicine by bringing together workstreams being undertaken by King’s College London, London, England, and 2 partners: the ICDAS Foundation and the ACFF. This undertaking has allowed ICDAS to lead the development of the International Caries Classification and Management System (ICCMS), which evolved through workshops held in several cities in Europe and the United States.24 In parallel, the ACFF and King’s College London led a series of 3 Dental Policy Labs that brought together disparate stakeholders to develop strategies for moving toward a cavity-free future.25 The project encompasses health, economic, and policy considerations, as well as paying for health in dentistry,26 and then moves toward oral and dental health through partnership27 by linking dental public health, behavioral change, and industry. The 2 strands then converge, with the development of the tailored version of ICCMS for practice known as the CariesCare International “4D” system.28,29 The strategy that emerged, with consensus from many contributors over 18 years, focuses on the preservation of tooth structure and allowing time for secondary prevention of caries to work. These integrated caries classification and management systems have led to a holistic, patient-centered, long-term view of caries control, monitoring, and outcomes.
Importance of early detection
Early detection of caries is important across multiple domains and is now seen as a vital part of caries assessments in both public health settings and clinical practices. Figure 5 illustrates the importance of early detection in terms of preservation of tooth structure and saving teeth, as well as its value in research, dental public health, clinical practice, and dental education. These approaches are embedded in the ICCMS system (which is now advocated by the FDI World Dental Federation30) and its goals, which center on preventing new lesions from appearing, preventing existing lesions from advancing further, and preserving tooth structure.24 The system and the approach used are also supported by a wider range of international evidence,31-36 including that for the problematic field of early childhood caries.37,38 In addition, and most importantly during the global COVID-19 pandemic, this preventive and minimally interventive strategy leads to fewer surgical interventions and consequently less aerosol generation.
Figure 5
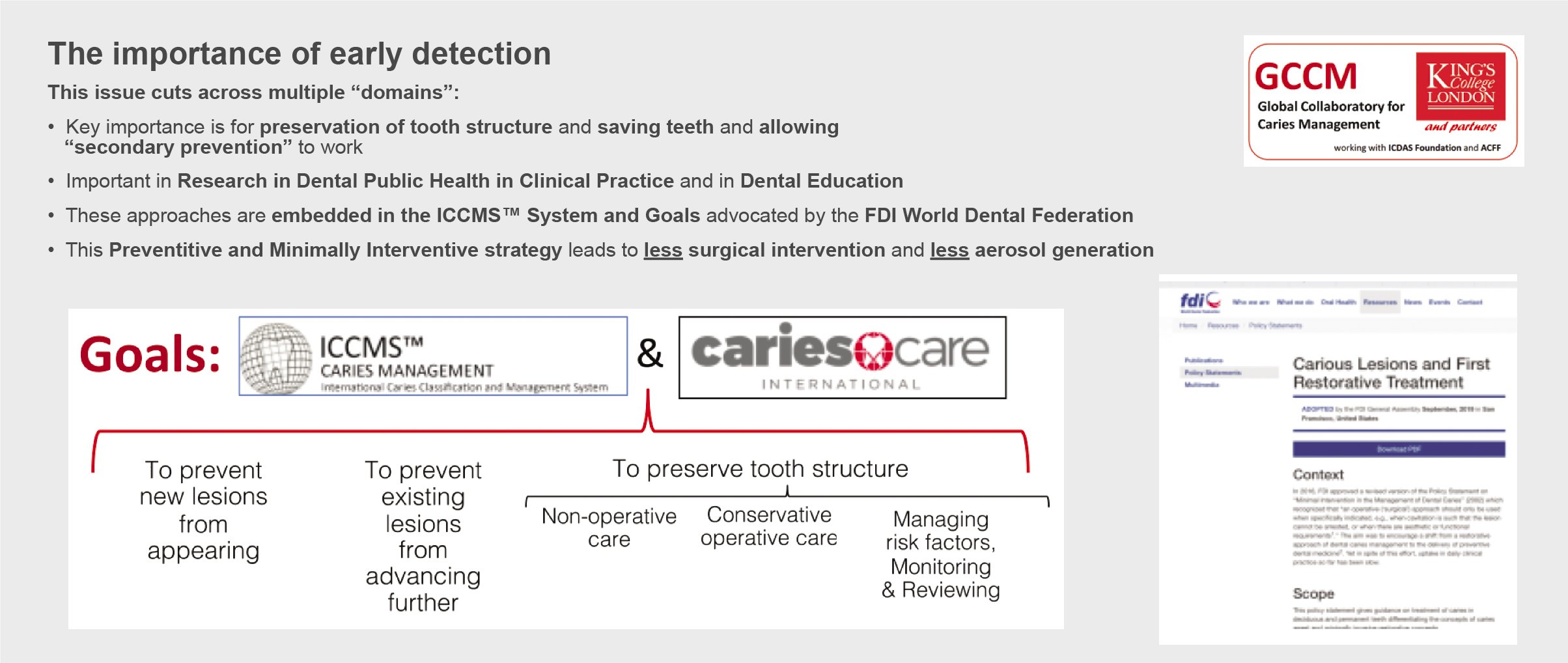
Pitts NB (Editorial). “ICDAS” - an international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate clinical management. Community Dental Health 2004; 21: 193-198Pitts NB and Zero D. FDI Word Dental Federation-Colgate Caries Prevention Partnership. White Paper on Dental Caries Prevention and Management. FDI Word Dental Federation, 2016, http://www.fdiworlddental.org/media/93783/2016-fdi_cpp-white_paper.pdf. Martignon S, Pitts NB et al. CariesCare Practice Guide: Consenus on Evidence into Practice. British Dental Journal. 227: 353-362, 2019. https://www.nature.com/articles/s41415-019-0678-8.
Related evidence-into-action activities
These findings from caries research have informed a range of evidence-into-action activities across 5 stakeholder domains. These are further research,4 clinical practice,28,29 dental education,39-41 public health,14 and policy.25-27 These activities have the potential to improve caries care in a post–COVID-19 world. To highlight 2 examples, let us consider implementation of ICCMS in clinical practice and the impact of the Dental Policy Labs.
Figure 6 illustrates the CariesCare International 4D system,28,29 which was developed by an international team to facilitate implementation of ICCMS into dental practice. The system aims to be practice-friendly and to guide the dental team and the patient through a 4-step cycle to improve health outcomes42:
- Determining caries risk
- Detecting and assessing each lesion
- Deciding on a personalized care plan for each patient
- Doing minimally interventive tooth-preserving care before using a risk-based recall to start the cycle again.
Figure 6
There is now international consensus on what needs to be implemented to use ICCMS™️in dental practice
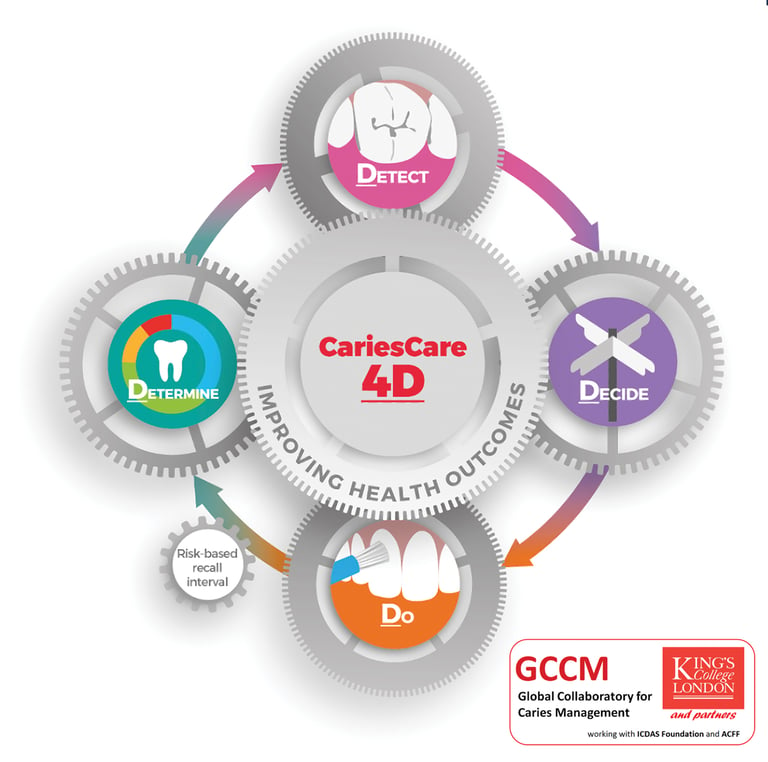
This 4D system is supported by an international consensus on evidence into practice (endorsed by 44 authors from 17 countries)28 and an illustrated case study.29 In addition, there is a dedicated website (https://cariescareinternational.com/) with access to documents, translations, lectures, and e-learning resources.
This work has generated 2 editorials in the British Dental Journal. In the first editorial, Hancocks43 supports the move to more preventive and less invasive care, argues that it should be paid for, and links the approach to the implementation of the United Nations Environment Programme International Minamata agreement, which seeks a global reduction in the use of mercury and consequently the international phase down of the use of dental amalgam. The author suggests that CariesCare could lead the way toward “minimal intervention dentistry” globally. The second editorial by Hancocks44 was published shortly after the international lockdown associated with the COVID-19 pandemic. He somewhat bravely explored inconsistencies in the attitudes with which the public and profession view health and disease, looked at the burdens associated with untreated dental caries, and contrasted them with both coronavirus and contaminated water. Citing a Dental Policy Lab meeting27 and the CariesCare International 4D system,28 Hancocks opined that the recent dramatic global changes in behavior due to the pandemic may lead to a situation in which stakeholders such as governments, societies, populations, and individuals can work collaboratively to control caries. For at least 17 years, the dental community has been asking itself if we are ready to move from operative to nonoperative/preventive treatment of dental caries in clinical practice,45 and the COVID-19 pandemic just may provide the stimulus for widespread change.
In a guest editorial, Klemmedson46 pointed out that the COVID-19 pandemic has led to a “renewed opportunity to emphasize prevention and to promote indications for noninvasive caries management.” In addition, during the pandemic, an international group adapted CariesCare International protocols for use in children. It shared knowledge and experiences across countries and centers using teledentistry and a range of nonaerosol-generating procedures and published a 1-year “Caries OUT” multicenter single-group interventional study protocol.47
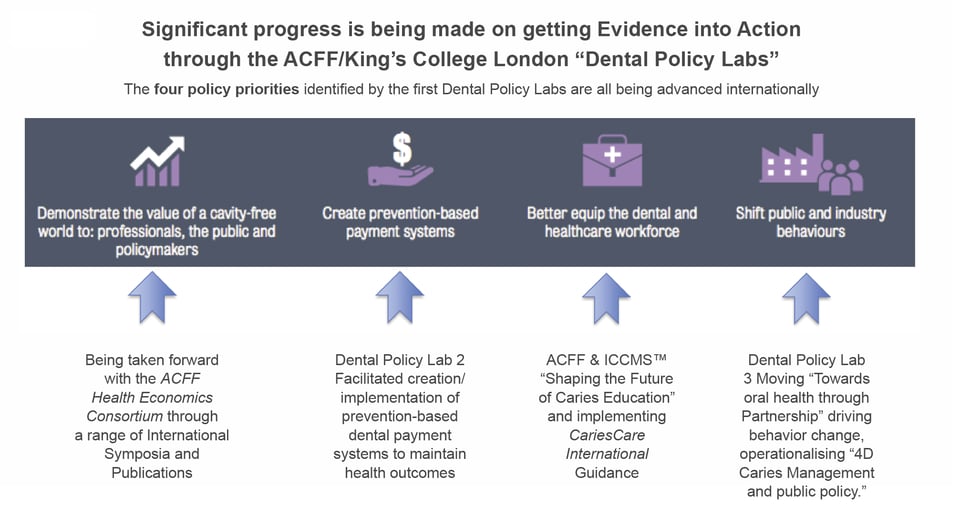
Figure 7 summarizes the significant progress being made in getting evidence into action through the ACFF/King’s College London Dental Policy Labs. The 4 priorities identified by the first Dental Policy Lab25 are being advanced internationally. These actions are to (1) better demonstrate the overall and economic value of a cavity-free future, (2) create prevention-based payment systems, (3) better equip the dental and health care workforce, and (4) shift public and industry behaviors. The lab participants, who come from many diverse stakeholder groups, developed recommendations that have had a substantial impact, and the ACFF/King’s College London Oral Health Policy Lab Network is currently being established to allow implementation experiences to be shared and the wide range of key recommendations to be advanced.25-27 In addition, the Making Cavities History global consensus policies18,19 facilitated by ACFF can now be used globally and locally to help implement the 2021 recommendations of the WHO resolution on oral health, the first to be issued in 14 years.48
Figure 7
CONCLUSIONS
Integration of new and existing concepts of caries affects how we refer to it, detect it, and prevent and control it. These concepts also impact our assessment of how and when we should intervene surgically. At a time of dramatic change, these insights offer new ways in which caries prevention can be achieved and care can be provided for populations and individuals to maximize health
outcomes and minimize both surgical intervention and generation of aerosols.
Acknowledgments
The author gratefully acknowledges all who have contributed to this long, complex, and continuing caries journey:
- all at the Faculty of Dentistry, Oral & Craniofacial Sciences,
- King’s College London, London, England, the ICDAS Foundation Board, and the ICDAS Coordinating Committee;
- those who have helped with ICCMS and CariesCare International;
- those who have joined with us from other organizations around the world;
- all at the Alliance for a Cavity-Free Future, and Colgate supporters;
- and all others who have provided financial and intellectual support for our work on caries.