This article explores why the complementary mechanisms of action of fluoride and arginine have been shown to be a winning combination as an anticaries agent.
ABSTRACT
Globally, an estimated 2 billion people experience caries of permanent teeth and 514 million children suffer from caries of primary teeth. The use of fluoride as a caries preventive agent continues to be the primary preventive strategy deployed in the fight against caries worldwide. However, based on the persistent high caries rates and for some populations, especially in areas of the world where endemic fluorosis exists, it is prudent to continue to explore the potential for new actives and strategies for caries prevention. The most widely studied alternative preventive strategy which has been identified utilizes the naturally occurring amino acid, arginine, as a prebiotic to enhance the mouth’s natural defense mechanism against caries by helping to maintain plaque pH in a neutral state while maintaining or fostering the return to a healthy microbiome. As the use of non-fluoride toothpastes, with no known actives to address caries, continues to grow, arginine may be a choice that is equally as effective at preventing caries albeit by a different mechanism than fluoride. The complementary mechanisms of action of fluoride to strengthen the enamel and arginine to restore the microflora and oral environment to a healthier state have been shown to be a winning combination demonstrating superior efficacy and the best caries prevention results reported in the literature thus far.
(The articles in this JADA+ series on arginine were presented at a symposium and did not undergo peer review.)
Introduction
For over 60 years, since the advent of the first mass-marketed toothpaste in 1955, the majority of caries prevention strategies have been centered around the use of fluoride. This strategy focuses on making the tooth more resistant to acid damage by allowing for the replacement of the hydroxyl ions in hydroxyapatite with fluoride-forming fluorapatite, resulting in increased hardness of tooth mineral. The topical application of fluoride also enhances tooth remineralization. The use of fluoride is not unwarranted; clinical studies support significant reductions (23%) in caries incidence with fluoride use,1 and the FDA recognizes several fluoride sources as generally safe and effective for the prevention of caries. However, even with the use of fluoride, caries as a disease remains prevalent today, affecting 60% to 90% of all schoolchildren and the vast majority of adults.2 Furthering this point, the World Health Organization Global Oral Health Status Report (2022) estimated that oral diseases affect close to 3.5 billion people worldwide, with 3 out of 4 people affected living in middle-income countries.3 Globally, an estimated 2 billion people suffer from caries of permanent teeth and 514 million children suffer from caries of primary teeth. This number is staggering and makes caries twice as common as headaches.4
Based on these early findings, the use of fluoride as a caries preventive agent continues to be the primary preventive strategy deployed in the fight against caries worldwide. However, based on the persistent high caries rates and for some populations, especially in areas of the world where endemic fluorosis exists, it is prudent to continue to explore the potential for new actives and strategies for caries prevention. Furthermore, in addition to areas of the world where endemic fluorosis is a concern, there has also been a growing consumer segment that actively seeks alternatives to fluoride products to sustain their oral health. These consumers have become concerned with multiple sources of fluoride ingestion and the potential health outcomes that could arise with exposure to excessive fluoride. Regardless of whether these concerns are justified, they have become an important consideration for consumers when choosing over-the-counter caries prevention products for themselves and their families. An increasing number of consumers choose to brush with fluoride-free alternative toothpastes, believing that these products present a viable alternative for caries prevention while addressing their perceived concerns about the safety of fluoride.5 A recent evidence-based review supports the use of fluoride-free toothpastes as cleaning agents to remove debris in the oral cavity and to potentially reduce gingivitis while emphasizing the fact that toothpastes without a caries preventive active such as fluoride have failed to show a benefit in terms of reducing the incidence of dental caries.6 To address these aforementioned concerns and findings, an effective alternative to fluoride has been explored and studied alone and in combination with fluoride, as it is clear that fluoride alone has been unable to address the significant burden of caries worldwide.
The most widely studied alternative preventive strategy that has been identified utilizes the naturally occurring amino acid, arginine, as a prebiotic to enhance the mouth’s natural defense mechanism against caries by helping to maintain plaque pH in a neutral state while maintaining or fostering the return to a healthy microbiome. Unlike fluoride, which has a chemical mode of action that targets the tooth, arginine is metabolized by arginolytic bacteria through the Arginine Deiminase System (ADS), which produces ammonia, helping to modulate the pH and resulting in a more neutral environment, shifting the dysbiotic microbiome to one that is healthier and less caries-prone.7,8 To date, numerous clinical studies have been conducted with toothpastes containing arginine at various levels (typically 1.5% to 8%). While arginine with calcium carbonate was at first most widely used in dentistry to occlude dentin tubules to prevent sensitivity, arginine is now proving to be a new and useful active in controlling caries. Arginine is a natural, safe amino acid found in saliva as well as in food products, dietary supplements, baby food, formula, and breast milk. It is not surprising that arginine is found at higher concentrations in the saliva of people who are caries free versus the low levels detected in people with a history of dental decay.9,10 It appears to be our body’s own protective measure against caries. This review will focus on results from key clinical trials that have explored the use of arginine (in the presence of a calcium source) as an anticaries agent (with and without fluoride), laying the foundation for future studies to support this new caries preventive agent as an alternative and/or complementary choice to be considered in our fight against caries.
Arginine with Fluoride
Research on arginine combined with fluoride has been conducted based on years of in vitro and in vivo research. The combination of arginine to address pathogenic microbial shifts with fluoride known to strengthen the enamel and to make it more resistant to decay addresses 2 processes across the caries continuum, which clinically has been proven to be more effective than focusing on a single process. In this combined strategy, arginine acts through targeting bacteria that are implicated in caries development, while fluoride helps by strengthening enamel and remineralizing surfaces of the teeth that had become compromised.
Years of research on arginine combined with fluoride has given support for dual use. The body of work for arginine plus fluoride, while not as extensive as fluoride alone, is by no means small; in total, over 25 clinical studies have been conducted on this technology (Table 1). Clinical research in this area of arginine with fluoride has been conducted over a decade and has included over 18,000 subjects. Clinical studies on arginine and fluoride can be classified into 4 types: plaque metabolism, microbiome, in situ intraoral, and caries assessments. The results from these studies, taken in aggregate, support the use of arginine and fluoride to achieve an additive, if not synergistic, effect on caries prevention far exceeding previous clinical results seen with fluoride alone. In addition, these studies clearly demonstrate the ability of arginine, a newly identified active against caries, to make substantial contributions to caries prevention strategies. A summary table of key arginine plus fluoride clinical studies is included in Table 1.
Figure 1
Benefits of adding a modern approach to traditional approaches for caries management
Plaque Metabolism Studies
As previously mentioned, throughout the history of caries prevention, the bulk of applications have been centered around fluoride and its ability to harden weakened enamel. However, there has been a movement to address the microbes and acidic environment that initiates the caries process, resulting in caries prevention strategies that focus on the source of caries, pathogenic plaque bacteria. Arginine has been studied to determine if it can produce a healthier microbial environment by limiting acidogenic bacteria while favoring arginolytic base–producing bacteria.7,11,12 In Wolff’s study, participants in the test group brushed for 2 weeks with a dentifrice containing 1.5% arginine and 1450 ppm fluoride.11 This arginine and fluoride toothpaste was shown to significantly increase plaque’s ability to convert arginine to ammonia relative to brushing with a control dentifrice containing only 1450 ppm fluoride. The resting pH, which is plaque’s natural pH in the absence of a sucrose challenge, of both the arginine plus fluoride and the control fluoride groups was also examined. Typically, resting pH ranges from 6.8 to 7. Under resting pH conditions, plaque is supersaturated with respect to enamel and there is a positive driving force favoring remineralization. An increase in resting pH increases the degree of saturation of the plaque fluid with respect to enamel and increases the force behind enamel remineralization. It was observed that the resting pH of the group who used the arginine- and fluoride-containing toothpaste was significantly higher than the group using the control fluoride product at the end of the 2-week treatment period (P ≤ 0.01; 7.31 for the arginine/fluoride group versus 7.1 for the fluoride group). This result signals that enamel remineralization would be favored in the arginine and fluoride group over the fluoride alone control group.
In Situ Intra-Oral Studies
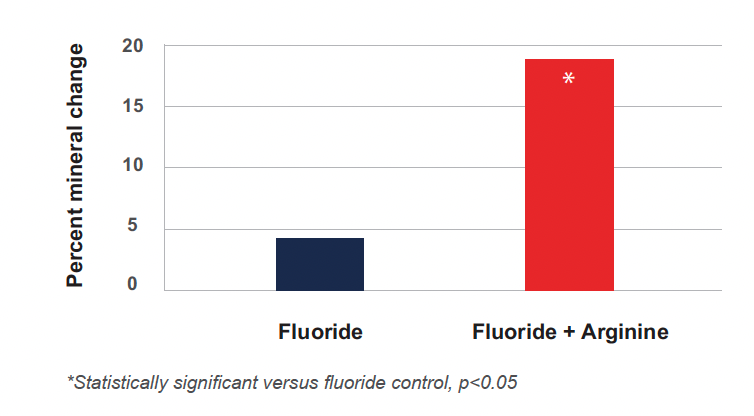
Another way of assessing the ability of dentifrices to remineralize tooth structure and to withstand demineralization in vivo is to observe their performance during in situ intraoral studies. These studies are typically designed to assess either remineralization–demineralization (remin-demin) or demineralization–remineralization (demin-remin). Remin-demin studies measure mineral gain to a surface, whereas demin-remin studies examine mineral loss or demineralization. A remin-demin clinical model was used to assess the ability to promote remineralization of enamel by 2 dentifrices containing different formulations of 1.5% arginine and 1450 ppm fluoride, as sodium monofluorophosphate (MFP), relative to a positive control with dicalcium phosphate dihydrate (Dical) and 1450 ppm fluoride and a negative control with Dical and 250 ppm fluoride.12 Microradiography and image analysis were used to measure mineral changes. The study used a double-blind crossover design with a 2-week treatment period. Products were used twice a day for 2 weeks. The percent mineral changes were +18.64, +16.77, +4.08, and −24.95 for the 1.5% arginine/Dical/1450 ppm fluoride, the 1.5% arginine/calcium carbonate/1450 ppm fluoride, the positive control with 1450 ppm fluoride alone, and negative control with 250 ppm fluoride alone, respectively. The positive control was statistically significantly better than the negative control in promoting remineralization (P = 0.0001), which indicates the study results are valid. The 2 arginine-containing test products showed statistically significant benefits beyond the positive control (P < 0.05) (Figure 2). No significant difference was observed in efficacy between the 2 arginine- plus fluoride-containing products, indicating that efficacy in promoting remineralization was independent of the choice of dical or calcium carbonate as the source of insoluble calcium in the formula.
Figure 2
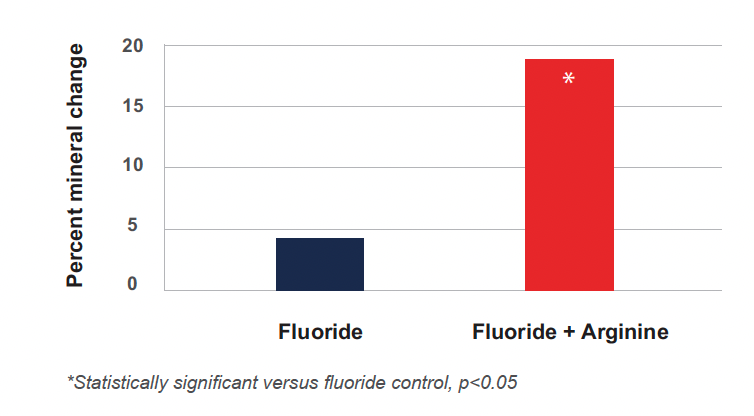
Arginine significantly enhances remineralization as shown in Cantore 2013
In a demin-remin study, a dentifrice containing 1.5% arginine, dicalcium phosphate dihydrate, and 1450 ppm fluoride was compared to matching positive and negative controls with 1450 ppm and 250 ppm fluoride, respectively, as was described in Cantore.12 Net mineral loss was experienced for both positive and negative controls. The observation that the positive control was statistically significantly more effective in preventing mineral loss than the negative control validates the benefits of the arginine technology. The percent demineralization values were −8.50, +1.67, and +12.64 for the 1.5% arginine/Dical/1450 ppm fluoride, the positive control, and negative control dentifrices, respectively. No net mineral loss was experienced following the use of the arginine- plus fluoride-containing dentifrice; enamel specimens actually showed an increase in hardness after the treatment period. Importantly, the arginine- plus fluoride-containing dentifrice was shown to be statistically significantly more effective than the matched positive control dentifrice in preventing demineralization of enamel. These results indicate that arginine is playing a significant role in enhancing the efficacy of fluoride.
Caries Studies
There are a number of studies with fluoride and 1.5% arginine that look closely into how these ingredients may impact the caries continuum. Early caries lesions were assessed using the quantitative light-induced fluorescence method.13-15 Arginine and fluoride, when formulated in a dentifrice, showed 2 times the reversal of early caries lesions as compared to 1450 ppm fluoride alone (Figure 3).
Longer studies on fluoride and arginine dentifrices have also been conducted, all demonstrating the improved efficacy of arginine and fluoride toothpastes against caries.16 In one 2-year study, a double-blind, randomized, unsupervised, parallel-group clinical trial on over 5,500 children in China on the efficacy of arginine and fluoride was demonstrated.17 In this study, the 2 test dentifrices contained 1.5% arginine, 1450 ppm MFP, and an insoluble calcium compound, whereas the positive control dentifrice contained 1450 ppm fluoride in a silica base. The children were examined at baseline as well as 1 and 2 years after continuous product usage. After 1 year of use, there were no statistically significant differences among the 3 groups with respect to decayed, missing, and filled teeth (DMFT) or to decayed, missing, and filled surfaces (DMFS). However, after 2 years of product use, subjects in the 2 test groups using the dentifrices containing arginine had a statistically significant reduction in DMFT increments of 20.5% and in DMFS increments of 19.6% when compared with subjects in the group using the positive control dentifrice with fluoride (Figure 4). Importantly, there were no statistically significant differences with respect to DMFT or DMFS between the 2 test groups containing arginine, showing that both formulations were effective.
Figure 3
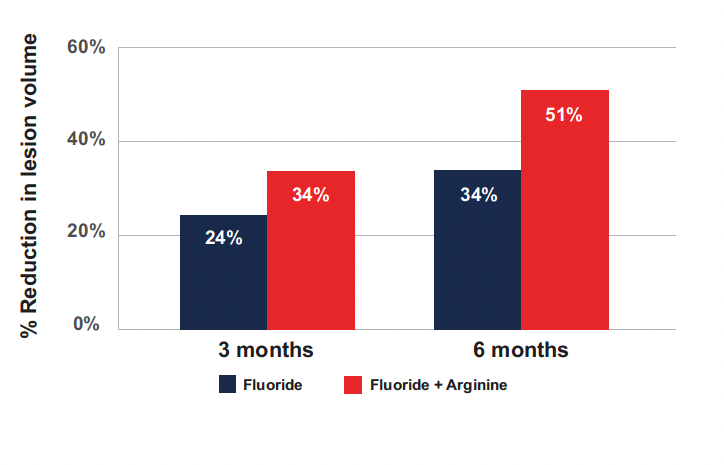
Reduction in lesion volume for Fluoride and Fluoride + Arginine at 3 months and 6 months as shown in Yin 2013 b. 34% reduction in caries volume was seen at 3 months for the arginine and fluoride combination dentifrice compared to a 34% reduction seen after 6 months of fluoride alone dentifrice use. Comparatively, at 6 months, the arginine and fluoride dentifrice had a 51% reduction in lesion volume demonstrating the additive effect of combining arginine with fluoride (Yin, 2013a; Yin, 2013b).
Figure 4
Arginine + Fluoride: superior reduction in caries, 24 month caries clinical
Microbiome Studies
A growing number of clinical studies have shown that the key to controlling caries may lie in the ability to foster a microbial community in the oral cavity that is resistant to caries. More specifically, microbes with the Arginine Deiminase System (ADS) have been shown to play a role in caries resilience. Arginine found naturally in the saliva is broken down, primarily by the ADS, which is found in arginolytic bacteria within oral biofilms, to produce ammonia. Ammonia production increases the pH, which inhibits tooth demineralization by neutralizing glycolytic acids and which stabilizes the biofilm community, enabling the survival of the good bacteria or commensals and suppressing the emergence of a cariogenic microflora while also helping to maintain supersaturation conditions for enamel, favoring remineralization. Notably, the ADS has been found to be active in some commensal Streptococcus species such as S. sanguinis and S. gordonii.18
It has been known for some time that caries-free individuals have higher pH levels and elevated ammonia levels compared with people with caries—both at rest and after a carbohydrate challenge.19-22 Arginine serves as a prebiotic, providing nutrition for the beneficial bacteria and weakening the effect of caries-causing bacteria, helping to restore the dysbiotic microflora to a healthy microflora, protecting the caries sufferers. Clinical work by Nascimento explored the impact of adding exogenous arginine on ADS activity, which was measured by the quantification of ammonia produced within oral samples at baseline, after a washout period, after 4 weeks of treatment, and 2 weeks after treatment.23 In this study, the treatment was a 1.5% arginine-only dentifrice, which was compared to an 1100 ppm fluoride toothpaste in 19 caries-free (DMFT = 0) and 19 caries-active (DMFT > 2) individuals. These studies demonstrated that Arginine increased the ADS activity levels and shifted the flora of caries-active individuals toward a flora more typical of caries-free individuals.23 More recently, Zheng showed that treatment with a dentifrice containing 8% arginine plus 1450 ppm fluoride helped to normalize the oral microbiome in caries-active individuals.24 It was found that after treatment, the microbiome of the caries-active individuals became more similar to the caries-free individuals, the enzymatic activity associated with acid production was reduced, and the alkali-generating enzymes and corresponding transcripts were enhanced. Another notable finding from this study was that S. sanguinis, which is an ADS-containing bacteria, was enriched, whereas the acidogenic/aciduric S. mutans was suppressed. With this important shift in bacteria, the demineralizing capability of the biofilm was substantially reduced.
Caries: Arginine Only Studies
As previously mentioned, there are subsets of the population across the world that would benefit from alternatives to fluoride dentifrices. In certain regions where there is a high level of naturally occurring fluoride, endemic fluorosis remains a problem, while in other parts of the globe, there is a strong consumer preference for anticaries solutions that do not include fluoride. For both these populations there exists a strong unmet need for an effective anticaries dentifrice that is formulated without fluoride. While the body of clinical knowledge on arginine without fluoride is more limited, it is growing. Evidence shows that arginine when formulated without fluoride still exhibits an anticaries effect clinically. With multicenter clinical studies underway in both the United States and China, this body of evidence is certain to expand over time.
The Impact of an Arginine Dentifrice on the Development of Dental Caries in Venezuelan School Children
A double-blind proof of concept study was conducted over a 2-year period to assess the effect of an arginine-containing dentifrice on caries development in 11- to 12-year-old Venezuelan children.25 A total of 726 children were enrolled in the study, with 601 (304 test subjects and 297 control subjects) completing the study. The test group received a dentifrice containing 1.5% arginine, while the control group used a commercially available sodium fluoride 0.24% (1100 ppm fluoride) dentifrice. All subjects were instructed to brush 3 times a day for 1 minute followed by swishing for 30 seconds with their randomly assigned dentifrice.
Examination of caries prevalence was conducted using the DMFS caries index as the scoring method and the criteria reported by Radike, with the avoidance of any forceful probing of suspected noncavitated pits and fissures for caries lesions.26 After 6 months, the mean DMFS scores increased only slightly from baseline in both groups: 6.93 ± 0.22 (mean ± SEM) in the control group and 6.59 ± 0.22 in the test subjects. After 1 year, the mean DMFS score in the control group rose to 8.00 ± 0.24, and at 2 years, it leveled off at 7.92 ± 0.30. In contrast, the mean DMFS score in the test group using the arginine dentifrice decreased to 5.50 ± 0.24 after 1 year before rising to 6.99 ± 0.28 at the 2-year time point. Using the method of repeated measures analysis of variance adjusting for baseline values, the DMFS difference between the 2 groups was statistically significant at both the 1-year (P < 0.001) and 2-year (P < 0.024) time points when looking at premolars and second molars. This study showed that, after 2 years of use, a 1.5% arginine toothpaste was at least as effective as a 0.24% sodium fluoride (1100 ppm fluoride) toothpaste in reducing the formation of caries.
Enhancing ADS Activity through Exogenous Arginine
Beyond toothpastes containing arginine, the effect of introducing exogenous arginine through mint confections on dental caries has also been examined.27 This second proof of concept study was conducted to determine if a sugarless mint containing an arginine bicarbonate calcium carbonate complex is capable of preventing the development of dental caries in the primary molars and first permanent molars of 10.5- to 11-year-old Venezuelan children. The population enrolled had at least some caries in their primary or permanent teeth as evidence of caries activity. They were all instructed to continue their daily hygiene regimens with fluoride-containing toothpastes at 1450 ppm fluoride, and they were also exposed to fluoride through the National Salt Fluoridation Program. A total of 200 children were enrolled in this 1-year study, with 100 in the test group administered 2 mints with the arginine bicarbonate calcium carbonate complex twice daily and 100 in the placebo control group administered the sugar-free mints minus the active. The results supported previous findings, showing 75.6% fewer caries in the arginine test group than in the placebo control group of children after 6 months and 50.7% fewer caries after 12 months in the first permanent molars and some early erupting premolars and second molars.27 (Acevedo, 2008).
These 2 proof of concept studies along with the additive and synergistic benefits demonstrated in the arginine plus fluoride studies were the basis for the large multicenter studies ongoing in the United States and China to determine the efficacy of the active arginine delivered in toothpastes on caries prevention.
Looking Forward, Concluding Thoughts
Caries remains the most common chronic condition faced by humankind worldwide. Fluoride over the past 65 years has been effective at keeping caries rates at lower levels than we might see otherwise, but the caries burden worldwide remains high despite current preventive strategies. Fluoride is delivered in various ways: toothpastes, mouthrinses, varnishes, gels, tablets, and in many water supplies as a public health effort to prevent caries. But it clearly has not resolved the issue, as diet and nutrition are also important in any risk-reduction strategy. The development of additional new actives can also help to alleviate this global oral health issue. Arginine is a new active to use in the battle against caries, with a growing body of evidence both preclinically and clinically for the use of this natural prebiotic to aid in caries prevention strategies.
In addition, addressing the microbiome is an essential element to consider in prevention strategies and when treating caries. Our oral microbiome is acquired at infancy. We know that children with poor oral health and dietary habits are more likely to develop cavities. The development of caries in the deciduous or primary teeth sets the course for the continued development of caries in permanent teeth. A child with an unhealthy microbiome is at risk for oral health problems as an adult. Arginine found within saliva, breast milk, baby formula, and healthy baby foods serves as a natural prebiotic to help maintain a healthy microbiome.
As consumer sentiments change, we must have all the tools available to us to combat caries. As the use of nonfluoride toothpastes, with no known actives to address caries, continues to grow, arginine may be a choice that is equally as effective at preventing caries, albeit by a different mechanism than fluoride. The complementary mechanisms of action of fluoride to strengthen the enamel and arginine to restore the microflora and oral environment to a healthier state have been shown to be a winning combination, demonstrating superior efficacy and the best caries prevention results reported in the literature thus far. Fluoride and a new active arginine offer the practitioner and consumers multiple options, including fluoride alone, arginine alone, or the combination of the 2, based on choice and caries risk. Beyond the exploration of additional new actives to address caries, it is also clear that sugar consumption, poor oral hygiene, and access issues need to be addressed as well in our fight against caries.
Dr. Ryan is Vice President and Chief Clinical Officer of Colgate Palmolive Company, New York, NY.